Topics
- Article
- Member Stories
- Organizations
A Doctor's Heart Rate While Saving a Life & Combating Stress in the Intensive Care Unit
About a year ago, I had the most memorable night of my internal medicine residency--and probably the most memorable night of my entire life.
I was nearing the end of my day in the Intensive Care Unit (ICU). Just before evening sign-out, one of the patients started to decompensate, aka get very sick very quickly. For the next several hours time stood still, and I remember every second like it was yesterday.
It Started with a Heart Rate Spike...
The elevated heart rate was consistent with a rhythm that we call atrial fibrillation, and sometimes this fast heart rate can cause blood pressure to drop (as there is not enough time for the heart to adequately fill to eject enough blood to support the body). Fortunately, the rate spontaneously normalized, but only transiently. Soon the monitor showed rates into the 200s and blood pressure was rapidly dropping.
We “shocked” the patient (synchronized cardioversion) to try to break the abnormal rhythm, to no avail. He then lost pulses and the rhythm was no longer shockable, therefore chest compressions were initiated. After two rounds of CPR and pushing epinephrine, we got him back.
The room was calm. The teamwork was flawless. Everyone was performing their tasks swiftly, and without hesitation. Things were stable, but we were not out of the woods. It was unclear what led to this acute change.

We went back to the drawing board. What brought him into the hospital in the first place? What workup had been done? What could we be missing? It was a very complex case, with multiple consultants giving their input, yet no one could pinpoint an issue. The cardiology team, hematology/oncology team, infectious disease team, and ICU team were going back and forth on all the potential causes. We were stumped.
Being the senior resident in the ICU, I led the discussions with the family in the waiting room to review everything that happened, everything that we knew, and everything that we were doing. They were grateful for all of the care from everyone – the nurses, respiratory therapists, social workers, residents, fellows, and attendings. It really was a team effort.
As physicians, we devote our lives to taking care of sick patients in hopes of making them better, this instance was no different. We worked tirelessly to stabilize this crashing patient and, fortunately, things started to settle down. Or so it seemed…
Back to Square One
The patient was already intubated (breathing tube in place to control breathing, on a ventilator). Next, his blood pressure dropped. We adjusted his medications, but there was little effect. He was nearly on every “pressor” (medications that help clamp down the blood vessels in order to increase blood pressure) we had. We increased them as high as they would go. No improvement. His heart rate soon doubled, and we prepared to shock him again. It worked. Things were briefly stable, but without identifying and treating the underlying cause, they would not stay like that for long.
Five minutes later, we lost pulses again. An unorganized rhythm was present on the monitor, but it was one that would not respond to another cardioversion (shock). Chest compressions were started again, and epinephrine was given at scheduled intervals – we call this “coding” a patient – performing CPR and giving certain medications based on Advanced Cardiac Life Support (ACLS) algorithms.
After 3 rounds of CPR, we re-established a pulse. He was back. The situation had finally settled down, and it stayed that way. Everyone was elated. Soon, the family was able to spend time with their father/husband/brother in a stable setting. The code was successful. Everyone regrouped and celebrated this victory, that we were able to sustain life even when it seemed to be hopeless. It was truly remarkable.
Life is a Beautiful Thing
Saving a life is a surreal feeling that I cannot even begin to describe. Nothing will supersede the face on the patient’s wife when I could finally deliver the news that we were successful in all our resuscitation attempts. I would be lying if I said I didn’t share a tear with the family.
Afterwards I sat down and decompressed, recounting everything as we documented the sequence of events. The ICU team had a huddle and discussed what aspects went well, and where we could improve – a critical and undervalued part of training – asking the hard questions like “How can we do this even better?”
Everyone had something to learn, and we all walked away better than when they started. Medicine truly is a career filled with life-long learning, and experiences such as this one can really shape your outlook. I was humbled that we could come together and save this man’s life, and always will be.
My Own Elevated Heart Rate
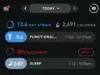
As I was walking out of the hospital, I received a notification on my phone from WHOOP: “Your activity is ready for review.” This was odd, as I clearly had not been at the gym, nor had I been physically exerting myself. But when I opened up the app and looked at my heart rate during this “activity,” I was quite shocked at what I saw:

I’d spent 57 minutes at an average heart rate of 143, with a max heart rate of 173. It looked just like I was working out, but I wasn’t. To recap, I had not been doing chest compressions or any actual physical or strenuous activity, aside from standing at the bedside of the patient and running the code. However, it was clear that my heart rate was quite responsive to the elevated stress in the moment.
This really got the wheels in my brain turning… In medicine, stressful times like these are more common than not, and it is clear that remote monitoring of physiologic metrics could capture this stress in real time (seen here by heart rate elevation in a high-stress scenario).
Quantifying the Stress of Medical Training
My next question was: Can we utilize this strategy to determine the stress of medical training on a larger scale? Could we determine when and where the stress on trainees was the greatest, and hope to find ways to improve stress levels during these times? What else can we learn about cumulative stress on the body and its effects on physiologic metrics such as heart rate variability, resting heart rate, REM sleep and deep sleep?
I slept on this idea. And by slept, I really mean “slept,” as it was more of a nap. After leaving the hospital I went to the gym to blow off some steam from the evening’s events. I got to bed a little after 1:00 am and was up a few hours later to be back in the ICU by 6:00 am.
Not surprisingly, my WHOOP recovery was 20% and my sleep duration was suboptimal as well. Regardless, I was there to work hard the next day and give it my all, something that I strive to do every day, no matter what. This is part of the grind of residency.
A few weeks later, near the end of the month-long stint in the ICU, I was looking at my WHOOP data and noticed some interesting trends. My sleep duration and restorative sleep (REM and deep sleep) were some of the lowest they'd been in 3 years. I'd averaged 4 hours and 58 minutes of sleep per night for the past 30 days, with just 1:08 of REM and 1:01 of deep sleep. Those restorative sleep numbers were roughly half of my averages throughout residency.
My heart rate variability, a marker of not only physical but also mental and emotional stress on the body, was also at an all-time low for a 30-day stretch (47) and my average resting heart rate was up significantly.

It was clear that my body was showing a physiologic response to what I was putting it through (a ton of stress). Interestingly, I was doing my best to take care of myself. I was eating the same, training at the gym the same, and (trying) to get as much sleep as I could. In reality the only variable that was added to the equation was the additional stress of being in the ICU work environment.
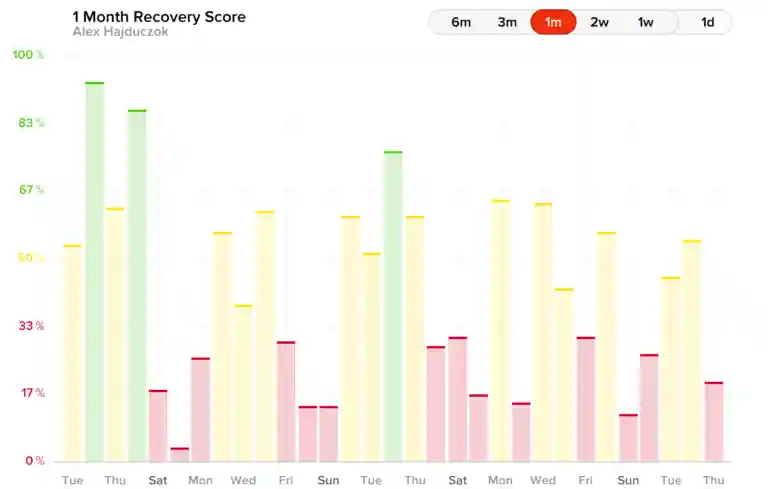
Even using all the optimization techniques I could, I still was consistently getting low recoveries (see all the red below). It dawned on me that we could use these metrics to track stress in medical training and apply this to burnout prevention.
A Study to Measure Resident Wellness & Prevent Burnout
I proposed this idea to one of my mentors (and one of the assistant program directors of our Internal Medicine residency program), Andrew Tinsley, and showed him the data that I had pulled together through 18 months of residency. It suggested some moderate correlations between work hours, HRV, RHR, and sleep. My other takeaway from the graph was how I needed to sleep more and work on improving my recoveries by optimizing HRV and RHR.

Fast-forward several months, and we were able to make this idea a reality, and now are approaching the half-way mark of the 12-month study using WHOOP to track resident wellness and burnout. I look back on how far we have come, and although there is much work to be done to make changes in medical/residency training, I believe we are on the right track to make improvements.
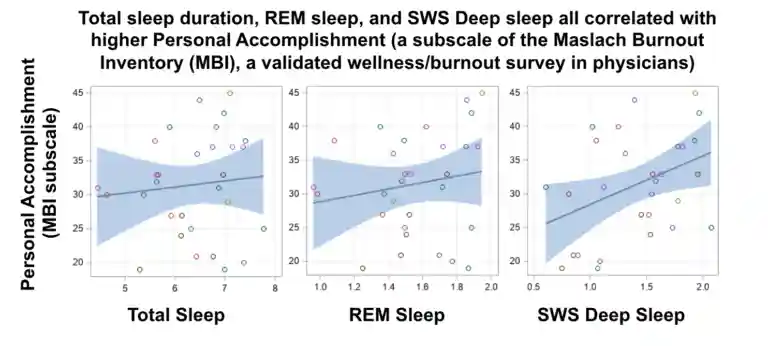
Nowadays, I am more focused than ever on how to make small changes in my daily habits to improve how I feel on a regular basis, as this directly translates to better performance in the hospital or outpatient setting. We have seen a close association between how people feel, how they perceive stress that they are under, and their physiologic metrics. Notably, our preliminary data shows tight correlations between increasing total sleep duration, REM and deep sleep, and improving physician wellness.
Although work hours might be a constant (bordering on 80 hours per week, or more, sometimes), there are other ways to stay healthy and it is still possible to thrive even in difficult circumstances. Hydration, stress reduction techniques (mindfulness, journaling, breathing exercises), sleep optimization strategies (sleep masks, blackout curtains, weighted blankets, no screens in bed), mitigation of unnecessary caffeine use, amongst other things, all seem to improve recovery.
We are excited to formally share the cumulative data at the conclusion of the study with the medical and scientific community in hopes of eliciting major changes in residency programs nationwide.
I have since rebounded from those long days in the ICU and have tried to utilize what I’ve learned in my research to improve my own wellness. I look forward to building on my experiences in training in fellowship, to continue working to find ways to enhance individual performance of physicians, and to hopefully provide avenues for the betterment of the medical community as a whole.
RELATED: 30 Murphs in 30 Days & What I Saw in My WHOOP Data
Events have been modified to protect patient confidentiality. The products and services of WHOOP are not medical devices, are not intended to diagnose COVID-19, the flu or any other disease, and should not be used as a substitute for professional medical advice, diagnosis or treatment. All content available through the products and services of WHOOP is for general informational purposes only.
Learn more about WHOOP for Healthcare here.
Learn more about how WHOOP Unite can support clinician wellness.